- Modifier 59 breaks NCCI procedure-to-procedure (PTP) edits when two codes describe genuinely separate, distinct services on the same date.
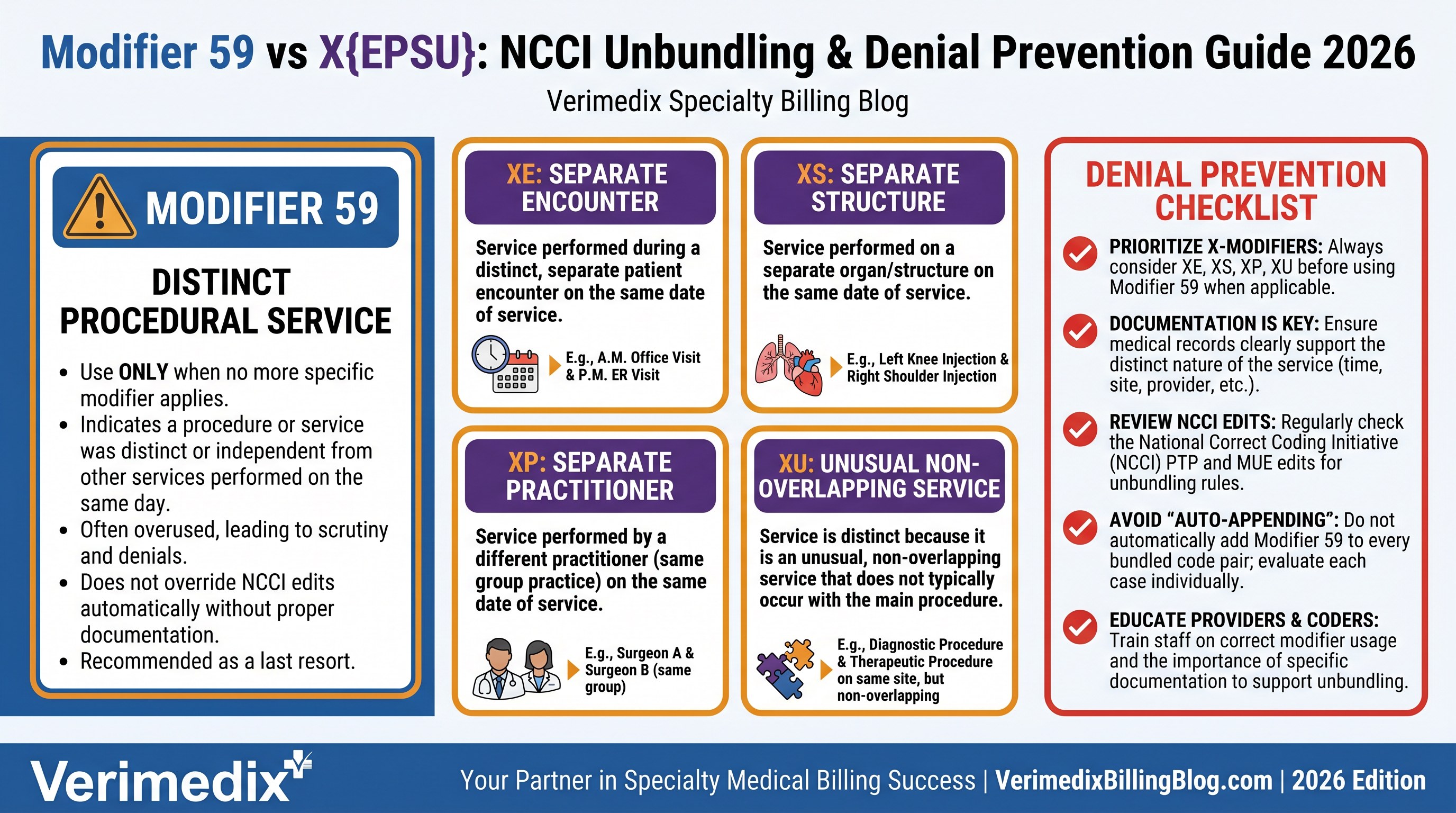
- X{EPSU} modifiers (XE, XP, XS, XU) are CMS-defined subsets of modifier 59 — more specific, preferred by CMS, and required by some payers in place of 59.
- Modifier 59 applies only to procedure codes — never to E/M codes (use modifier 25 or 57 for E/M).
- Two NCCI edit indicator types exist: indicator 0 (cannot be bypassed) and indicator 1 (can be bypassed with the correct modifier).
- OIG and RAC auditors target high modifier 59 utilization — documentation must prove the distinct service, not just assert it.
Modifier 59 is defined by AMA CPT as a distinct procedural service — a procedure or service not normally reported together with another code but which, under the circumstances, must be reported separately. CMS and its contractors use the National Correct Coding Initiative (NCCI) to publish quarterly-updated Procedure-to-Procedure (PTP) edit tables listing which code pairs are bundled and whether modifier 59 (or an X-modifier) can override the bundle.
How NCCI edits work
NCCI PTP edits pair a Column 1 code (the comprehensive service) with a Column 2 code (the component service). When both appear on the same claim for the same patient on the same date, the payer automatically bundles them and pays only the Column 1 code. Each edit carries a modifier indicator: 0 means the bundle cannot be broken regardless of documentation; 1 means the edit can be bypassed with the appropriate modifier when clinical circumstances genuinely support separate reporting.
CMS updates NCCI edits quarterly, so a pair that was unbundleable last quarter may be locked this quarter. Always verify the current NCCI table on the CMS website before billing a modifier-59 pair. Medically Unlikely Edits (MUEs) — which limit the number of times a code may be billed per date — are separate from PTP edits and cannot be bypassed with modifier 59.
When modifier 59 is correct
Modifier 59 is appropriate when two procedures are billed together but represent a distinct procedural service because they occurred at a different session or patient encounter; different anatomic site or organ system; separate incision or excision; separate lesion; or a separate injury not ordinarily encountered or performed on the same day. The modifier attaches to the Column 2 (component) code, not the comprehensive code. Documentation must independently support the distinct service — notes that blur both procedures together will not survive an audit.
The X{EPSU} modifiers: when CMS prefers them over 59
In 2015, CMS introduced four HCPCS modifiers as subsets of modifier 59 to provide greater specificity. CMS still accepts modifier 59 in most cases but may selectively require an X-modifier for code pairs at high risk for incorrect billing. Some Medicare Administrative Contractors and commercial payers have begun requiring X-modifiers in place of 59 for specific code pairs.
| Modifier | Full name | Use when the distinct service is because… | Example |
|---|---|---|---|
| XE | Separate Encounter | It occurred at a completely separate encounter the same day | Morning hospital visit + afternoon office procedure |
| XP | Separate Practitioner | It was performed by a different practitioner | Surgeon performs procedure; separate provider performs the imaging interpretation |
| XS | Separate Structure | It was performed on a separate organ or anatomic structure | Lesion destruction on left arm and right forearm, same date |
| XU | Unusual Non-Overlapping Service | The service does not overlap the usual components of the main service | Diagnostic colonoscopy plus a separate upper endoscopy that shares no overlapping work |
When an X-modifier precisely describes the reason for the distinction, use it instead of — or in addition to — modifier 59. Check your MAC's LCDs and your payer contracts, as specific code pairs may be listed with a required modifier type.
Modifier 59 vs. other modifiers
| Modifier | Applies to | Purpose | When NOT to use 59 |
|---|---|---|---|
| 59 / X{EPSU} | Procedure codes | Bypass NCCI PTP edit for distinct procedural service | Never on E/M codes |
| 25 | E/M codes only | Separate significant E/M on same day as minor procedure | Do not use on procedure codes |
| 51 | Procedure codes | Multiple procedures, same session — reduces additional procedure payment | Do not substitute for 59 when an NCCI edit is the issue |
| 76 / 77 | Procedure codes | Repeat procedure same day, same or different provider | Not for unbundling — use when repeat is clinically necessary |
Common modifier 59 denials and how to fix them
| Denial | Root cause | Fix |
|---|---|---|
| CO-97 (bundled into primary procedure) | NCCI edit with modifier indicator 1 — modifier 59 missing or documentation insufficient | Append modifier 59 or appropriate X-modifier to Column 2 code; submit distinct clinical notes for each service |
| CO-4 (modifier required) | Edit pair has indicator 1 but no modifier was appended | Add correct modifier; verify which modifier the payer requires (59 or X{EPSU}) |
| CO-97 sustained after appeal | Documentation does not support distinct service | Resubmit with separate procedure notes for each service; include date, site, and clinical necessity for each code |
| MUE denial (exceeds unit limit) | Modifier 59 does not override MUEs — only appended to same-line code | Resubmit with separate claim lines using the appropriate place-of-service and date; MUE appeals require medical records, not modifier changes |
Audit red flags to avoid
- High modifier 59 rate. OIG and RAC audits target providers whose modifier 59 usage significantly exceeds specialty peers.
- Modifier 59 on every claim. Routine use without individualized documentation signals upcoding.
- Modifier 59 on E/M codes. It cannot be used for E/M unbundling — that is modifier 25 territory.
- Using 59 to bypass indicator-0 edits. Those edits are absolute; no modifier overrides them.
- Missing separate notes. Both procedure records must exist independently in the chart, not as a single combined note.
Correct modifier 59 use is not just a reimbursement issue — it is a compliance issue. The documentation should make the distinction obvious to any reviewer before the modifier is appended, not after a denial letter arrives.
Frequently asked questions
Modifier 59 broadly identifies a distinct procedural service. XE (separate encounter), XP (separate practitioner), XS (separate structure), and XU (unusual non-overlapping service) are more specific CMS-defined subsets of modifier 59. CMS prefers the X-modifiers for greater precision and may require one instead of 59 for high-risk code pairs. When an X-modifier fits, use it.
No. Only edits with modifier indicator 1 can be bypassed with modifier 59 or an X-modifier. Indicator 0 edits are absolute — no modifier will override them. Medically Unlikely Edits (MUEs) also cannot be bypassed with modifier 59.
No. Modifier 59 is for procedure codes only. For a significant, separately identifiable E/M performed the same day as a minor procedure, use modifier 25. For an E/M resulting in the decision for major surgery, use modifier 57.
CO-97 after modifier 59 usually means documentation did not support a distinct service. Pull the clinical notes and confirm each procedure has its own separate, legible record showing a different site, session, or non-overlapping service. Write a concise appeal letter citing the NCCI indicator and attaching both procedure notes.
CMS updates NCCI Procedure-to-Procedure edits quarterly (January, April, July, October). A code pair that was unbundleable last quarter may have an indicator change in the new quarter. Always verify the current table on cms.gov before billing a modifier-59 pair.