- Modifier 25 flags a significant, separately identifiable E/M done the same day as a minor procedure (000/010-day global).
- Append it to the E/M code (e.g., 99213-25), never to the procedure code.
- The E/M must be above and beyond the usual pre/intra/post work bundled into the procedure.
- Use modifier 57 (not 25) for the E/M that prompts a major surgery decision (090-day global); modifier 59 is for procedures, never E/M.
- The fix for most denials is a clearly separate, legible note documenting distinct E/M work - a frequent OIG and payer audit target.
Modifier 25 is one of the most-used and most-audited modifiers in medical billing. It unlocks payment for an office visit performed the same day as a minor procedure - but only when the visit is genuinely separate work. This guide covers exactly when it applies, how it differs from modifiers 57 and 59, and the documentation that keeps it defensible.
What modifier 25 means
Per AMA CPT, modifier 25 is a significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of a procedure or other service. In plain terms: the provider did a real E/M visit and a minor procedure on the same date, and the E/M was significant and distinct from the work already built into that procedure.
CMS defines a minor procedure as one with a 000- or 010-day global period. The decision to perform that minor procedure is already paid inside the procedure, so a quick look before, say, draining an abscess is not separately billable. Modifier 25 applies only when the E/M is above and beyond that routine work.
How and when to append modifier 25
- Attach it to the E/M, not the procedure. Example: a patient presents for a planned lesion destruction but also reports new chest tightness - you report 99213-25 plus the destruction code.
- The E/M must stand on its own. It should reflect work beyond the usual evaluation tied to the minor procedure.
- A separate diagnosis helps but is not required. AMA and CMS confirm the E/M and procedure may share a diagnosis, but distinct chief complaints make the claim far stronger.
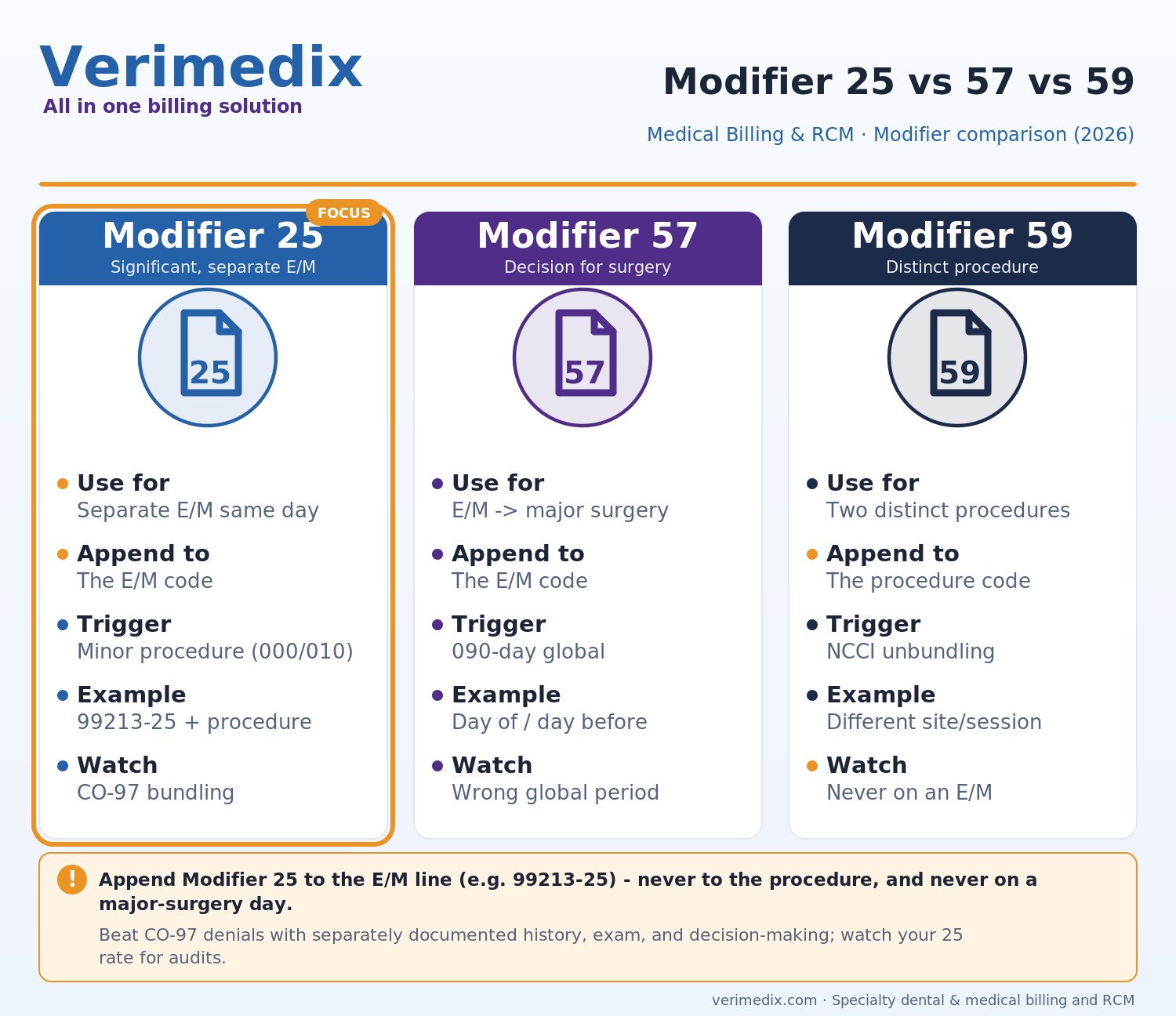
Modifier 25 vs. 57 vs. 59
| Modifier | Use it for | Applies to | Key trigger |
|---|---|---|---|
| 25 | Significant, separate E/M same day as a minor procedure | E/M code | Procedure has 000/010-day global |
| 57 | E/M that results in the decision for major surgery | E/M code | Procedure has 090-day global, decision day-of or day-before |
| 59 | Distinct procedural service (different site/encounter) | Procedure code (never E/M) | Unbundling two procedures per NCCI |
Bottom line: if the E/M prompts a major (090-day global) surgery, use modifier 57, not 25. Modifier 59 is an NCCI procedure-to-procedure modifier and should never be appended to an E/M service.
Common modifier 25 denials and how to fix them
| Denial reason | Why it happens | Fix |
|---|---|---|
| CO-97 (bundled / included in procedure) | Payer sees no separate E/M work | Submit a distinct note documenting separate history, exam, and decision-making |
| Payer downcoding | E/M level not supported by documentation | Match the E/M level to documented MDM or time; avoid reflexive 99214s |
| Overuse / audit flag | Modifier 25 on nearly every procedure visit (OIG scrutiny) | Append only when the E/M is truly significant; monitor your modifier 25 rate |
| Shared-diagnosis dispute | Payer wants a separate diagnosis | Link a distinct diagnosis when present; document why the E/M was separate even if shared |
| Modifier on wrong line | Modifier 25 placed on the procedure code | Re-bill with modifier 25 on the E/M line |
Common errors to avoid
- Putting modifier 25 on the procedure. It belongs on the E/M code, full stop.
- Using it for the decision to do a minor procedure. That work is already bundled into the procedure payment.
- Confusing it with modifier 57. Major surgery decision = 57; minor procedure same-day E/M = 25.
- Letting documentation blur together. The E/M and procedure notes must be clearly separate.
- Habitually appending it. A high modifier 25 rate invites OIG and payer audits - bill it only when earned.
Modifier 25 is worth real money when used correctly, and a real liability when it is not. The difference is disciplined documentation and clean claim construction across every encounter.
Frequently asked questions
Always to the E/M code, for example 99213-25. The procedure code stays unmodified. Placing modifier 25 on the procedure line is a common error that causes denials.
Modifier 25 is for a significant, separately identifiable E/M done the same day as a minor procedure (000- or 010-day global). Modifier 57 is for an E/M that results in the decision to perform a major surgery (090-day global), reported the day of or day before that surgery.
No. Both AMA and CMS allow the same diagnosis for the E/M and the procedure. However, a distinct diagnosis and clearly separate chief complaint make the claim much stronger and reduce the risk of a bundling denial.
CO-97 means the payer considers the E/M bundled into the procedure. It usually indicates the documentation did not show separate, significant E/M work. Fix it by submitting a distinct note with its own history, exam, and medical decision-making that stands apart from the procedure.
Only if the provider performed a significant, separately identifiable E/M beyond the vaccine counseling and administration. Appending modifier 25 to an E/M that exists solely to give a vaccine, with no separate evaluation, is a frequent audit target and will likely be denied.