- Modifier 24 reports an unrelated evaluation and management service by the operating surgeon during an active postoperative global period (10-day minor or 90-day major).
- Append modifier 24 to the E/M code, never to the surgery or procedure code.
- The visit must be genuinely unrelated to the original surgery — documented with a diagnosis that clearly diverges from the operative diagnosis.
- Modifier 24 is valid starting the day after the surgery through the end of the global period; on the day of surgery itself use modifier 25.
- Aftercare and surgical complication ICD-10 codes paired with modifier 24 will be denied by Medicare and most payers.
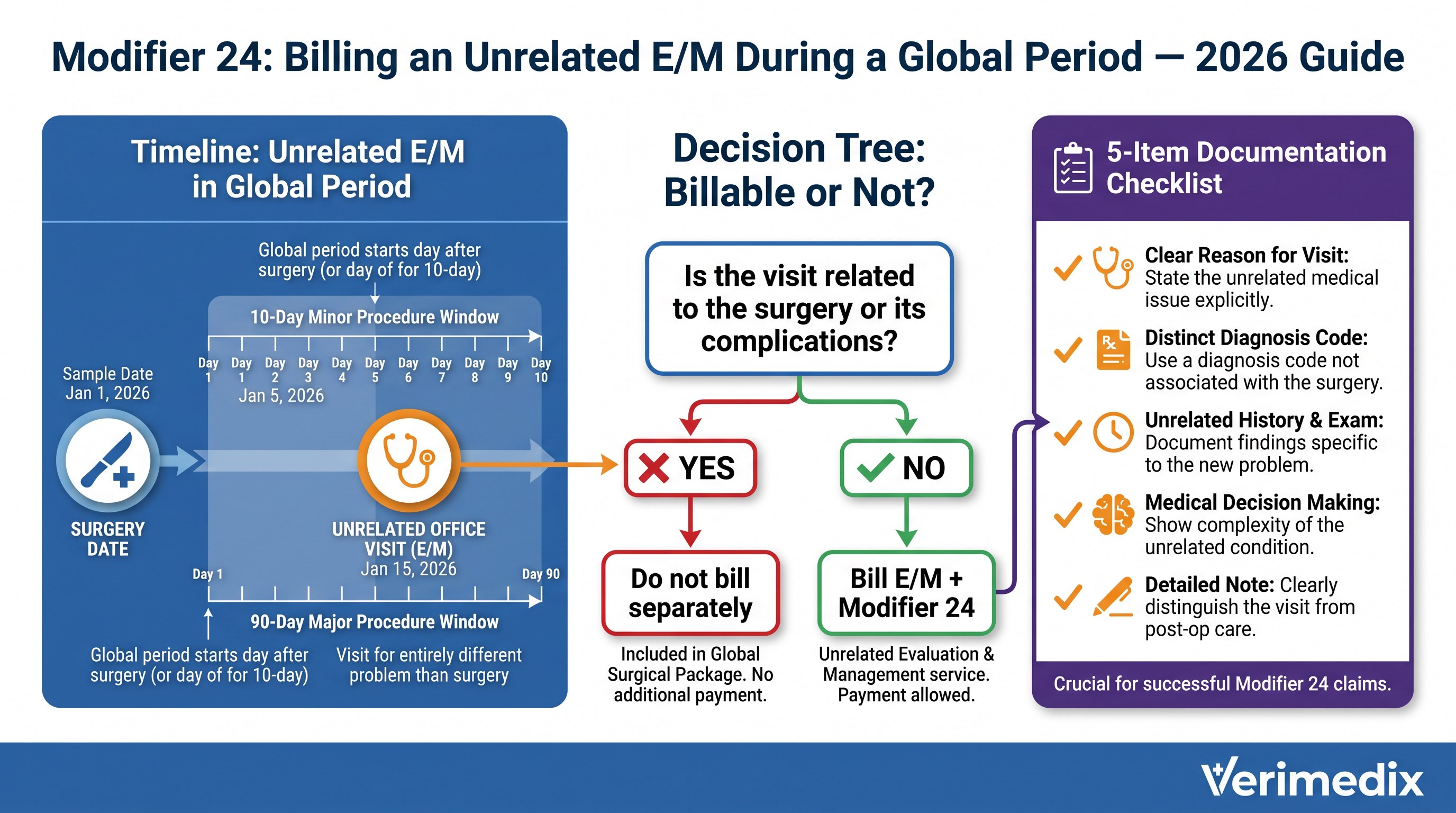
When a surgeon operates, a global surgical package automatically bundles all routine postoperative E/M visits into the procedure payment for the duration of the global period — 10 days for minor procedures and 90 days for major procedures. The only way to break that bundle for a genuinely separate problem is modifier 24. Without it, the E/M claim pays nothing regardless of the medical necessity of the visit.
Global period basics
CMS assigns every CPT surgery code one of three global period values: 000 (day of procedure only), 010 (day of and 10 days after), or 090 (day of and 90 days after). Routine follow-up care related to the surgery — wound checks, suture removal, expected recovery milestones — is already paid inside the procedure's RVU and cannot be billed separately. An evaluation for a completely new, unrelated medical problem is not bundled and must be separately reported with modifier 24.
When modifier 24 is correct
Modifier 24 applies when the operating surgeon sees the same patient during an active global period and the visit addresses a medical problem that is entirely unrelated to the original surgery. Classic examples include managing newly diagnosed hypertension discovered at a post-op visit, evaluating a contralateral limb injury unrelated to the operative site, or managing a pre-existing chronic condition such as diabetes during a 90-day orthopedic global period. The clinical record must document the separate chief complaint, a distinct problem-oriented examination, and an ICD-10 code that clearly does not arise from the operative episode.
The diagnosis requirement
CMS policy states that a visible signal that the visit is unrelated to the surgery is required. In practice this means attaching an ICD-10 code that bears no clinical relationship to the operative diagnosis. A different diagnosis code is not absolutely mandatory under AMA rules — but without one, a payer has no automated signal that the visit was unrelated, and the claim will typically deny. Aftercare codes (Z47.xx, Z48.xx), complication codes (T80-T88), and wound-care codes appended with modifier 24 will be denied by Medicare because they indicate surgery-related activity, not an unrelated problem.
Modifier 24 vs. 25 vs. 57
| Modifier | When to use | Timing | Applies to |
|---|---|---|---|
| 24 | Unrelated E/M during active postoperative global period | Day after surgery through end of global period | E/M code |
| 25 | Significant, separate E/M same day as a minor procedure (000/010-day global) | Day of the minor procedure | E/M code |
| 57 | E/M that results in the decision for major surgery (090-day global) | Day of or day before major surgery | E/M code |
Common modifier 24 denials and how to fix them
| Denial | Why it happens | Fix |
|---|---|---|
| CO-97 (bundled into global) | Modifier 24 not appended or documentation does not show unrelated visit | Append modifier 24 to the E/M code; attach visit note and distinct unrelated ICD-10 |
| CO-4 (modifier required) | E/M billed during global period without any modifier | Add modifier 24 and resubmit; confirm global period end date first |
| Denial — aftercare/complication diagnosis | ICD-10 signals surgery-related visit (T80-T88, Z47/Z48) | Correct the diagnosis to one that is clinically unrelated; if the visit was truly related, it is not separately billable |
| Denial — day of surgery | Modifier 24 used on the surgery date instead of modifier 25 | Replace modifier 24 with modifier 25 for same-day E/M; modifier 24 is valid only from the day after surgery onward |
| Payer requests medical records | High modifier 24 utilization triggers pre-payment review | Submit documentation proactively: note, unrelated diagnosis, and a brief narrative confirming no relationship to operative condition |
Documentation checklist
- Date of surgery and procedure code — to establish the global period start and end date.
- Separate chief complaint for the unrelated visit, clearly documented in the E/M note.
- ICD-10 code that is clinically unrelated to the operative diagnosis.
- Distinct history, exam, and medical decision-making (MDM) addressing only the unrelated problem.
- No wound-check, suture removal, or post-op follow-up language intermingled in the unrelated E/M note.
Modifier 24 is a legitimate and frequently underbilled tool. Many surgeons accept bundled global reimbursement for unrelated visits because they or their staff are unaware the modifier exists. A systematic chart review of global-period encounters often reveals recoverable revenue that was simply never billed.
Frequently asked questions
Not strictly required under AMA rules, but CMS and most payers expect an ICD-10 code that visibly signals an unrelated condition. Without a distinct diagnosis, the claim often denies because there is no automated signal the visit was unrelated to the surgery. Always use an unrelated diagnosis when one exists.
No. Modifier 24 applies starting the day after the surgical procedure through the end of the global period. For an unrelated E/M performed on the same day as a minor procedure, use modifier 25. Modifier 24 on the surgery date itself will be denied.
Yes. Modifier 24 is used by the operating surgeon billing during their own global period. A different physician who did not perform the surgery bills normally during the same period because the global package does not restrict other physicians’ billing.
The claim will pay initially but is a compliance risk. Auditors compare the visit diagnosis and note content against the operative diagnosis. If the visit is found to be related to the surgery, it must be repaid and may trigger broader scrutiny. Only append modifier 24 when the visit is genuinely, documentably unrelated.
Yes, provided the E/M is unrelated to the surgery and the telehealth rules (appropriate CPT code, place of service code 02 or 10, and any required telehealth modifier) are also met. The modifier 24 documentation requirements are the same regardless of visit modality.