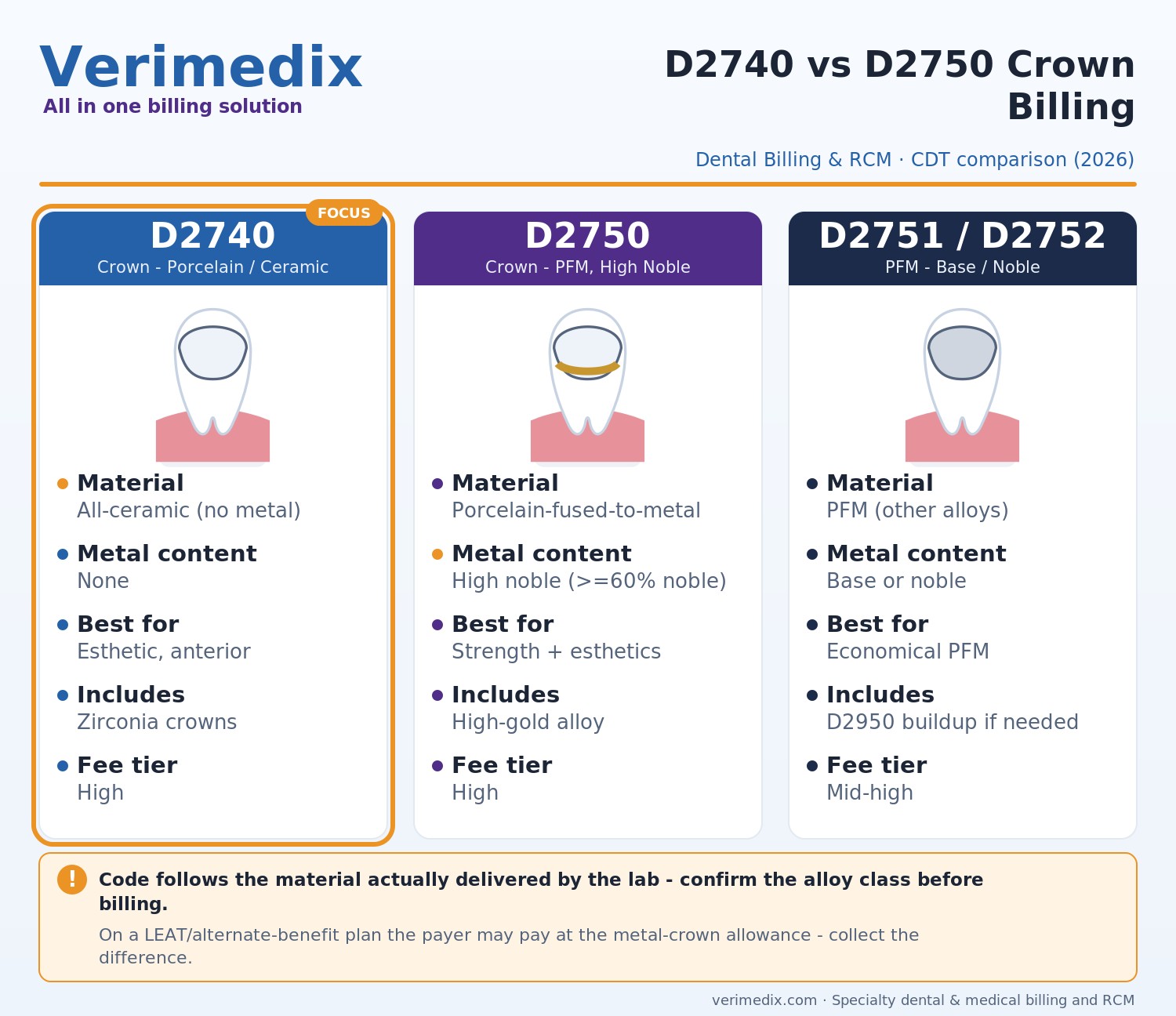
- D2740 = crown, porcelain/ceramic (no metal substructure); D2750 = crown, porcelain fused to high noble metal (PFM).
- The code is driven by the material actually delivered, not by what was planned at prep - confirm the lab material before billing.
- Many payers apply a LEAT (least expensive alternative treatment) or alternate-benefit downgrade on posterior teeth and pay a lesser fee; the patient owes the difference.
- Crowns typically carry a frequency limit of once per tooth every 5-7 years, and many plans require radiographs plus a narrative showing significant coronal destruction.
- The most common crown denials - missing radiographs/narrative, frequency, LEAT downgrade, and prep-vs-seat date mismatch - are all preventable.
Crown claims are some of the highest-dollar, highest-scrutiny line items in a dental practice - and two of the most confused codes are D2740 and D2750. Pick the wrong one, leave out a radiograph, or bill on the wrong date of service, and a high-value restoration stalls for weeks. This guide explains when each code applies, how alternate-benefit downgrades erode reimbursement, and how to build a clean claim.
D2740: Crown - Porcelain/Ceramic
Per the ADA CDT descriptor, D2740 is a single-unit crown made entirely of porcelain or ceramic with no metal substructure - including all-ceramic and contemporary monolithic or layered zirconia restorations. Use it for an esthetic, full-coverage crown on a natural tooth where the final restoration contains no metal. If a metal coping is present, D2740 is the wrong code. Note: D2740 is for a crown on a natural tooth, while D6740 is the analogous retainer crown on an implant or bridge - do not interchange them.
D2750: Crown - Porcelain Fused to High Noble Metal
D2750 is a porcelain-fused-to-metal (PFM) crown with a high noble metal substructure. Under ADA alloy classifications, high noble alloy must contain at least 60% noble metal (gold, platinum, palladium) with at least 40% gold. Because the code is tied to the alloy actually used, confirm the lab's material classification before submitting - billing D2750 on a base-metal coping is a misrepresentation that surfaces in audits.
D2751, D2752 and D2950: the codes that travel with crowns
| CDT code | Material | Typical use | Noble-metal content |
|---|---|---|---|
| D2740 | Porcelain/ceramic (no metal) | Esthetic anterior & posterior; zirconia | None |
| D2750 | PFM - high noble metal | Strength + esthetics, premium alloy | >=60% noble, >=40% gold |
| D2751 | PFM - predominantly base metal | Economical PFM | <25% noble |
| D2752 | PFM - noble metal | Mid-tier PFM alloy | >=25% noble |
| D2950 | Core buildup, including any pins | Rebuild lost coronal structure to retain a crown | N/A |
D2950 includes any pins by descriptor, so pins are never billed separately. A buildup is reimbursable only when there is insufficient remaining tooth structure for crown retention - not as a routine add-on to every crown.
LEAT and alternate-benefit downgrades
Many dental plans contain a least expensive alternative treatment (LEAT) or alternate-benefit clause. On posterior teeth, the plan may benefit a porcelain or PFM crown at the allowance for a less expensive metal crown - paying its share of the lower fee while the patient is responsible for the difference. A properly applied LEAT provision must be disclosed on the EOB and is a benefit determination, not true downcoding. The fix is financial transparency: verify the clause at eligibility, present a written estimate, and obtain signed financial consent before seating.
Documentation and frequency limits
- Diagnostic radiographs (current periapical and/or bitewing) showing the affected tooth.
- A clinical narrative describing the indication: significant coronal destruction, fracture, cracked-tooth syndrome, or a failed/recurrent restoration.
- Tooth number and surfaces, and the alloy class for the PFM codes.
Crowns carry a frequency limitation - commonly once per tooth every 5 to 7 years. A replacement crown inside that window needs a narrative documenting why. Confirm the exact frequency and any missing-tooth or downgrade clauses during eligibility, not after the seat.
Prep date vs. seat date
Payers are not uniform on the crown date of service. Some adjudicate on the preparation date, others on the seat (cementation) date. A mismatch generates a denial or an eligibility-lapse rejection if coverage changed between visits. Confirm each major payer's rule and standardize when your team drops the crown claim.
Common crown denials and how to fix them
| Denial reason | Why it happens | The fix |
|---|---|---|
| Missing radiographs/narrative | No supporting image or necessity statement | Attach current PA/bitewing plus a narrative citing destruction, fracture, or failed restoration |
| Frequency limitation | Replacement crown inside the 5-7 year window | Document the failure reason; verify frequency at eligibility before treatment |
| LEAT / alternate-benefit downgrade | Plan pays at a lesser metal-crown allowance | Disclose the clause pre-op; collect the signed difference; appeal only if misapplied |
| Prep-vs-seat date mismatch | Claim date conflicts with payer's required DOS | Use the payer-specific DOS rule; re-bill with the correct date |
| Code/material mismatch | D2750 billed on a base-metal coping | Confirm lab alloy class; bill D2751/D2752 as appropriate |
Frequently asked questions
D2740 is a crown made entirely of porcelain or ceramic with no metal substructure (including zirconia). D2750 is a porcelain-fused-to-metal crown built on a high noble metal coping (at least 60% noble metal, at least 40% gold). The code follows the material actually delivered by the lab.
Many plans apply a LEAT or alternate-benefit clause on posterior teeth, paying their share at a lower metal-crown allowance, with the patient responsible for the difference. Verify it at eligibility and obtain signed financial consent before seating.
Most plans impose a frequency limitation of once per tooth every 5 to 7 years. A replacement inside that window typically requires a narrative documenting the reason - fracture, recurrent decay, or a non-restorable failed crown.
No. D2950 is reimbursable only when there is insufficient remaining tooth structure to retain the crown. The descriptor already includes any pins, so pins are not billed separately. Pairing a buildup with a crown on a structurally intact tooth is a common audit and denial trigger.
It depends on the payer. Some adjudicate on the preparation date and others on the seat date. Using the wrong date causes denials or eligibility-lapse rejections. Confirm each major payer's rule and standardize your billing.