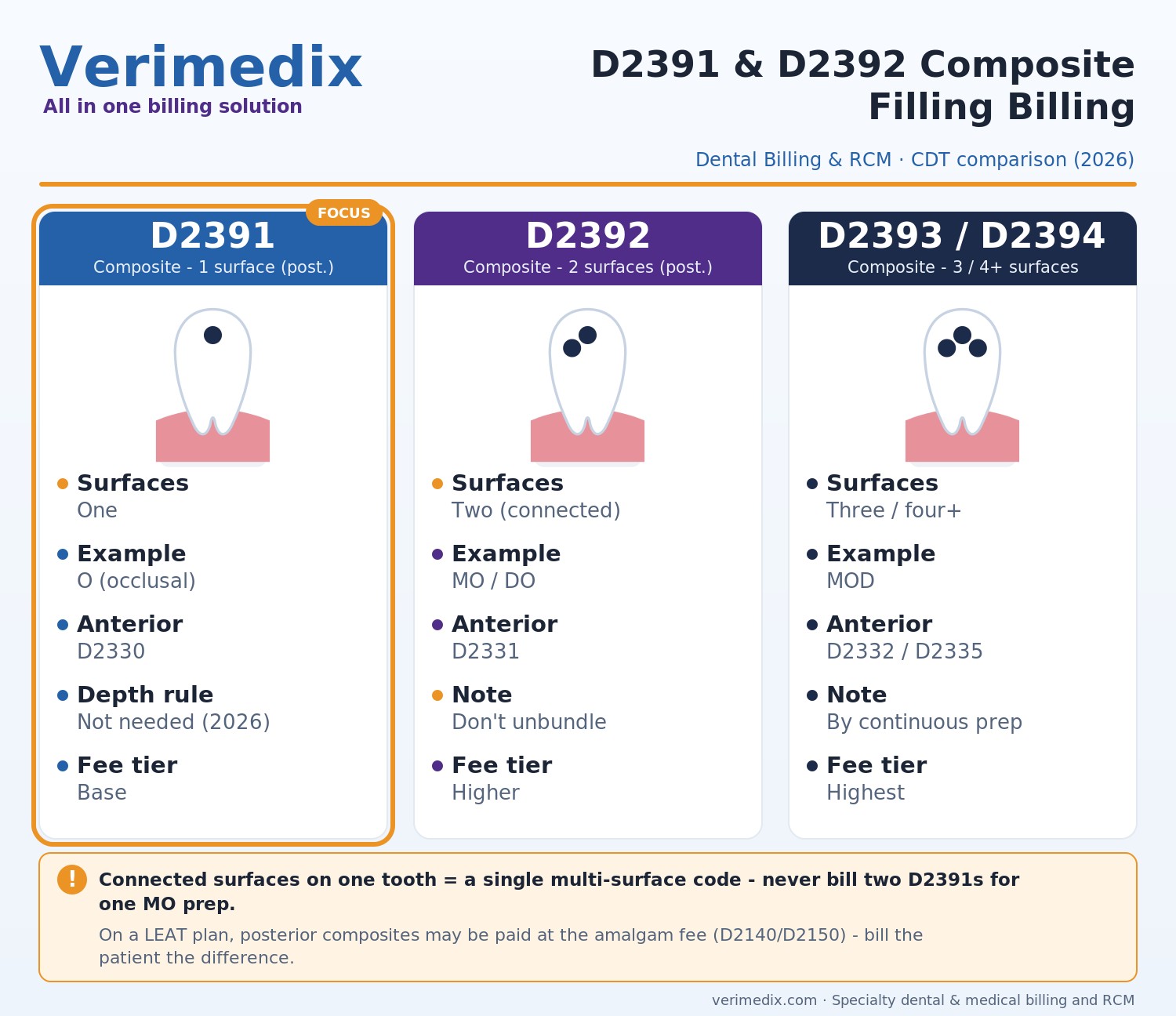
- D2391 = resin-based composite, one surface, posterior; D2392 = two surfaces, posterior. D2393 (three) and D2394 (four or more) continue the series.
- Connected surfaces on a single tooth are one multi-surface restoration - never bill two D2391s for an MO that is really one continuous preparation.
- Many plans apply an alternate-benefit (LEAT) downgrade, paying posterior composites at the amalgam fee (D2140/D2150 equivalent); the patient owes the difference.
- For 2026 CDT, the D2391 descriptor language limiting it to lesions into dentin was deleted - depth no longer drives code selection.
- Top denials: unsupported surface count, connected surfaces billed separately, misread alternate-benefit, and same-tooth/surface frequency conflicts.
Resin-based composite fillings are among the highest-volume restorative procedures in any practice, which is exactly why D2391 and D2392 generate so many denials. The codes themselves are simple, but payers scrutinize surface counts, apply alternate-benefit downgrades, and run frequency edits that quietly erode collections. Getting D2391 and D2392 composite filling billing right means understanding the surface anatomy, the plan's benefit design, and the documentation that ties them together.
D2391 and D2392 defined
Per the ADA's CDT code set, D2391 is resin-based composite - one surface, posterior, and D2392 is resin-based composite - two surfaces, posterior. Posterior means premolars and molars. The series continues with D2393 (three surfaces) and D2394 (four or more surfaces). For anterior teeth, use the parallel series: D2330 (one surface), D2331 (two), D2332 (three), and D2335 (four or more surfaces or involving the incisal angle).
One 2026 CDT update matters here: the historical D2391 descriptor language that tied the code to a restoration penetrating into dentin was removed. D2391 now reports a one-surface posterior composite regardless of how deep the lesion extends - but you still must document the surface accurately.
Surface-to-code reference table
| Surfaces restored | Posterior code | Anterior code |
|---|---|---|
| 1 surface | D2391 | D2330 |
| 2 surfaces | D2392 | D2331 |
| 3 surfaces | D2393 | D2332 |
| 4+ surfaces (or incisal angle, anterior) | D2394 | D2335 |
Tooth surfaces are reported with standard designators: M (mesial), O (occlusal), D (distal), B/F (buccal/facial), and L (lingual). A posterior MOD restoration is three surfaces (D2393); an MO is two (D2392); a single occlusal is one (D2391).
Surface counting: connected vs. separate
The governing rule: connected surfaces on a single tooth count as one multi-surface restoration, not multiple single-surface fills. If you restore a continuous mesial-occlusal lesion, that is one D2392 (two connected surfaces), never two D2391s. Unbundling connected surfaces is a fast track to a denial - and, in an audit, a refund request. Conversely, two genuinely separate, non-contiguous restorations on the same tooth can each be reported, with clear documentation showing they are independent.
Alternate benefit and the LEAT downgrade
Many dental plans contain an alternate benefit or least expensive alternative treatment (LEAT) clause for posterior composites. Under it, the plan pays D2391/D2392/D2393 at the corresponding amalgam fee - D2140 (one surface), D2150 (two surfaces), D2160 (three surfaces) - even though composite was placed. The composite is still a covered service; the plan simply benefits it at the lower amalgam allowance. The downgrade is not a denial and should not be appealed as one - the patient owes the difference. Disclose it with a signed treatment plan and verify the alternate-benefit language during eligibility.
Common denials and how to fix them
| Denial / scenario | Root cause | Fix |
|---|---|---|
| Surface count not supported | Documentation doesn't list the surfaces restored | Record M/O/D/B/L surfaces in the note; attach images; ensure the claim surface field matches the chart |
| Connected surfaces billed separately | Two D2391s submitted for one continuous prep (unbundling) | Report the single correct multi-surface code (e.g., D2392); rebill as a corrected claim |
| Paid lower than expected | Alternate-benefit/LEAT downgrade to amalgam fee | Don't appeal; bill patient the composite-to-amalgam difference per a signed agreement; verify language at eligibility |
| Frequency / same tooth-surface conflict | Same surface restored within the plan's replacement window (often 24-60 months) | Submit narrative explaining new decay, fracture, or failed prior restoration; attach radiographs |
| Tooth/surface mismatch | Code surface count doesn't equal surfaces listed | Align the code to the surfaces reported; correct the claim before resubmission |
Frequency limits and replacements
Most plans limit how often the same tooth or surface can be restored - commonly one restoration per surface every 24 to 60 months. When you must re-restore inside that window, document the clinical reason (recurrent caries, fracture, marginal breakdown, or failed prior restoration) and attach imaging. Verifying replacement frequency at the eligibility stage prevents the surprise entirely.
Frequently asked questions
D2391 is a resin-based composite filling on one surface of a posterior (back) tooth, while D2392 is a composite filling on two surfaces of a posterior tooth. The code is chosen by the number of connected surfaces actually restored in a single preparation.
Only if the restorations are genuinely separate and non-contiguous. If two surfaces are connected in one continuous preparation, you must report a single multi-surface code such as D2392 - billing two D2391s for connected surfaces is unbundling and will deny or trigger a refund request.
Most likely an alternate-benefit (LEAT) downgrade. Many plans pay posterior composites (D2391/D2392/D2393) at the equivalent amalgam fee (D2140/D2150/D2160). The service is still covered - the patient is responsible for the difference, which should be disclosed in a signed financial agreement.
No. For 2026, the ADA removed the descriptor language limiting D2391 to restorations penetrating into dentin. You report D2391 for a one-surface posterior composite regardless of lesion depth, but you must still document the surface accurately.
Record the specific tooth number and surfaces (M/O/D/B/L) in the clinical note, attach pre-operative radiographs, confirm the claim surface field matches the chart, and add a narrative for any replacement within the plan's frequency window.